Managing your Patients using the Information Prescription PLUS (Diabetes UK) Template
The Information Prescription PLUS (Diabetes UK) template is a simple to use screen that assists in meeting all of the Diabetes UK requirements for managing patients with Diabetes who are at risk of developing complications. The template includes:
- Up-to-date information viewable on one screen, including access to historical information
- Quick data entry functionality using the data entry tools
- A mail merge facility with direct links to the personalised Information Prescription plan which can be given to the patient
- Access to the Diabetes UK Care Pathway for Information Prescription

Below are some key points about using the Information Prescription PLUS (Diabetes UK) template:
Key Points
- Adding Data - To add data to the Information Prescription screen you can either use the Data Entry Tools at the end of each line. For a full explanation of all the options, see Using Templates.
- Viewing Data - The latest recorded entry displays on the template. To view historical data select Previous entries (red)
 . Previous entry (blue)
. Previous entry (blue)  icon indicates that the patient does not have any previous records.Note - All numerical results are also shown in a graph format at the bottom of the screen.
icon indicates that the patient does not have any previous records.Note - All numerical results are also shown in a graph format at the bottom of the screen. - Save and Close - All entries made to the screen should be saved by choosing the Save and Close
 icon. If you do not save and close your data will be lost.
icon. If you do not save and close your data will be lost. - QOF - A red Q
 in front of a line indicates this information is also required for QOF.
in front of a line indicates this information is also required for QOF. -
Links to the Information Prescription plan - The template contains quick links to the Information Prescription plan which allows the patient to see the targets they need to work towards to improve their condition as well as giving background information and the steps they should be taking to do this for improvement.
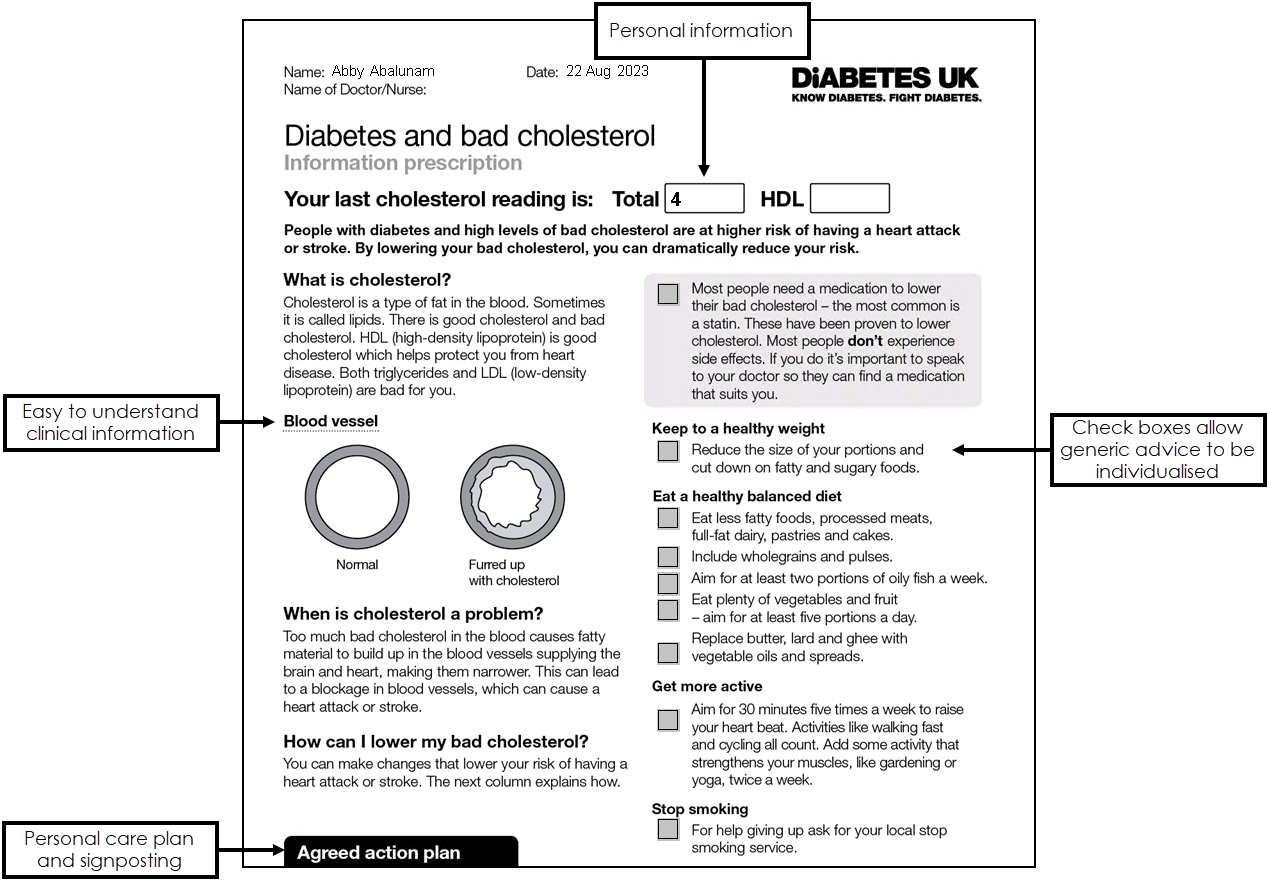
The Information Prescription plan opens in Microsoft Word with patient specific actual and target diabetic information automatically populated. You can also add additional comments, for example target settings and care planning. The Care plan includes:
- Personal Information
- Easy to comprehend clinical information
- Signposting and support information
- Personal care planning
- Actions to reduce risk
 Note - The Prescription Information plan is not saved in the patient's record, however you can clinical term that you have given the patient an Information Prescription by selecting the line labelled Information Prescription on the template.
Note - The Prescription Information plan is not saved in the patient's record, however you can clinical term that you have given the patient an Information Prescription by selecting the line labelled Information Prescription on the template. - Colour Coding on the Template - Text in green on the Prescription Information template indicates that the patient qualifies, for example they have Diabetes or they require an Information Prescription plan. Text in black indicates that data is missing. If you are not able to add data it means that the patient does not qualify for an Information Prescription.
- Diagnosis - Use this section of the screen to view or record the patient's Diabetes diagnosis.
- Blood Pressure - This area of the template enables you to view historical blood pressures or add a new blood pressure reading.
- Cholesterol - This part of the screen shows the patients latest cholesterol results. This information automatically populates from the clinical system or you can add a new result by selecting the data entry tools at the end of the line.
- HbA1c - This section of the template enables you to view the patient's latest HbA1c results. This information automatically populates from the clinical system or you can add a new result by selecting the data entry tools at the end of the line.
- Information Prescription - This line is present in each section of the template so that you can record that you have given the patient an Information Prescription plan. The clinical term 8CE - Self-help advice leaflet given is recorded in the patient's record.